Some quick notes on the importance of the pelvic floor and why the body's second diaphragm should be addressed during movement
Over the last 8 months, I have become fascinated by the role pelvic position plays on the body's stability. More accurately, I discovered the importance of the pelvic floor on all things low back oriented. I train many people that suffer from low back pain. some of whom have had surgery, others that are trying to avoid surgery. While many of them have positional similarities, the most striking similarity I have found (now that I know to look for it), is the inability to maintain pelvic position with activation of muscles that work in the transverse plane, such as the transverse abdominis and internal rotators of the hip. Once this is cued correctly and the person knows how to "find" the proper engagement, stability increases dramatically (and people feel their "core." It's pretty amazing). While there are often other things that need to be addressed in these clients to improve function, this is an incredible starting point. The senior yoga people have been trying to explain this to me for years; however, rather than explain the anatomy, they use mystical terms such as mola bandha. I think many of the advanced pilates/gyrotonics people might know this, but I have never been fully immersed in that world, so I can't speak for sure.
The pelvic floor is often considered the body's second diaphragm. When there is a physiological change in the diaphragm, either during inhalation, exhalation, or coughing, there is a symmetrical change in the pelvic floor activation (Bordoni and Zanier, 2013). In order for proper intra-abdominal pressure to be maintained during respiration, support from the pelvic floor is required. This ensures trunk stability, and corresponds to activity in the transverse abdominis and internal obliques- therefore, if your pelvic floor isn't working properly, your deep abdominal muscles probably aren't working properly, causing an alternative (and less efficient) stabilizing strategy.
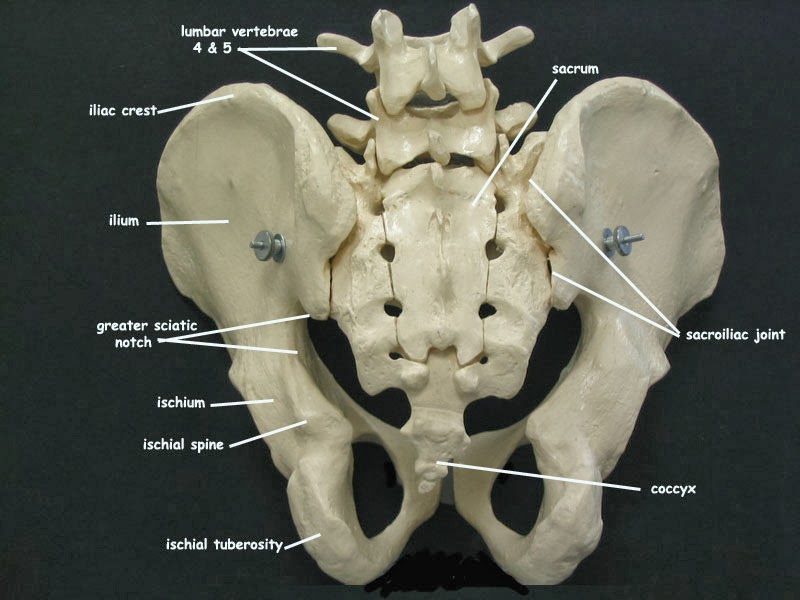
How does this relate to pelvis position? It is worthwhile to note that the pelvis is required to move in all three planes (sagittal, frontal, and transverse) during the gait cycle (Lee & Lee, 2011). The sacrum, which attaches to the pelvis at the sacroiliac joint, needs to nutate and counter-nutate during various movements. For the purpose of this blog, think of the sacrum as something that moves slightly to handle load dispersal. If the sacrum is unable to move because the pelvis isn't able to move in all three planes, load will not travel well up the spine. If, for instance, someone remains in an extended posture most of the time, the anterior inlet spills forward and abducts, and the posterior inlet moves backward and adducts (see picture below). Think of what happens to the sacrum if the pelvis is stuck in this position- it can't move and the muscles on the back of the pelvis (specifically the piriformis) are going to be "gripping" to keep a person upright. Further, the muscles in the pelvic floor are long and loose- they aren't able to provide the support needed for the bottom of the canister to co-contract and provide stability. This is going to lead to movement inefficiencies (and possibly SI joint "tightness" or pain). In this example, to move the pelvis to neutral, we need to inhibit the piriformis by activating the internal rotators of the hip, activate the hamstrings to pull the pelvis down in the back, and activate the transverse abdominis and internal obliques to pull the pelvis up in front. In a sense, we are mobilizing the pelvis so it can move more freely during the gait cycle. (For some ideas on how to work with someone in an extension pattern on co-activation of the muscles in the pelvic floor, see the video: http://youtu.be/UtJnY0MhIPA).

(The anterior pelvic inlet is labeled in the picture above. You can see how when the pelvis tips forward, it will give the appearance that the top portion of that circle is widening. Conversely, the posterior pelvic inlet, which would be the view from the back and can be seen in the picture below, will appear to narrow when the pelvis is tipped forward. If you look at where the SI joint is located, you will notice that if you tilt the pelvis forward, the sacrum won't have much room to move).
As I have mentioned before, I view my job as a movement professional to help people move as efficiently as possible. This is directly related to the body's ability to stabilize on the deepest level, and really, it means having an understanding of what is required for the body to do that. If the pelvic floor and the engagement of the deep abdominal muscles is ignored, performance will be hindered. The crazy thing is I have watched efficiency (and movement quality) improve dramatically in yoga practitioners, golfers, and triathletes by simply improving the function of the deep stabilizing system. I have also seen grandparents pick up their grandchildren without pain, and low back pain lessen. Anatomy and physiology in the absence of disease is consistent- understanding how the body works dynamically is the most valuable tool a movement professional can have.
Your in health and wellness,
Jenn
P.S.- If you find this topic interesting and would like to study it further, I highly recommend Diane Lee's work (her website can be found at http://dianelee.ca/index.php) and/or the Postural Restoration Pelvis course (either home study or live).
Bordoni, B., & Zanier, E., (2013). Anatomic connections of the diaphragm: influence of respiration on the body system. Journal of Multidisciplinary Healthcare, 6, pp. 281-291.
Lee, D., (2011). The Pelvic Girdle, Fourth Edition. Churchill Livingston Elsevier: Toronto.
The pelvic floor is often considered the body's second diaphragm. When there is a physiological change in the diaphragm, either during inhalation, exhalation, or coughing, there is a symmetrical change in the pelvic floor activation (Bordoni and Zanier, 2013). In order for proper intra-abdominal pressure to be maintained during respiration, support from the pelvic floor is required. This ensures trunk stability, and corresponds to activity in the transverse abdominis and internal obliques- therefore, if your pelvic floor isn't working properly, your deep abdominal muscles probably aren't working properly, causing an alternative (and less efficient) stabilizing strategy.
How does this relate to pelvis position? It is worthwhile to note that the pelvis is required to move in all three planes (sagittal, frontal, and transverse) during the gait cycle (Lee & Lee, 2011). The sacrum, which attaches to the pelvis at the sacroiliac joint, needs to nutate and counter-nutate during various movements. For the purpose of this blog, think of the sacrum as something that moves slightly to handle load dispersal. If the sacrum is unable to move because the pelvis isn't able to move in all three planes, load will not travel well up the spine. If, for instance, someone remains in an extended posture most of the time, the anterior inlet spills forward and abducts, and the posterior inlet moves backward and adducts (see picture below). Think of what happens to the sacrum if the pelvis is stuck in this position- it can't move and the muscles on the back of the pelvis (specifically the piriformis) are going to be "gripping" to keep a person upright. Further, the muscles in the pelvic floor are long and loose- they aren't able to provide the support needed for the bottom of the canister to co-contract and provide stability. This is going to lead to movement inefficiencies (and possibly SI joint "tightness" or pain). In this example, to move the pelvis to neutral, we need to inhibit the piriformis by activating the internal rotators of the hip, activate the hamstrings to pull the pelvis down in the back, and activate the transverse abdominis and internal obliques to pull the pelvis up in front. In a sense, we are mobilizing the pelvis so it can move more freely during the gait cycle. (For some ideas on how to work with someone in an extension pattern on co-activation of the muscles in the pelvic floor, see the video: http://youtu.be/UtJnY0MhIPA).
(The anterior pelvic inlet is labeled in the picture above. You can see how when the pelvis tips forward, it will give the appearance that the top portion of that circle is widening. Conversely, the posterior pelvic inlet, which would be the view from the back and can be seen in the picture below, will appear to narrow when the pelvis is tipped forward. If you look at where the SI joint is located, you will notice that if you tilt the pelvis forward, the sacrum won't have much room to move).
As I have mentioned before, I view my job as a movement professional to help people move as efficiently as possible. This is directly related to the body's ability to stabilize on the deepest level, and really, it means having an understanding of what is required for the body to do that. If the pelvic floor and the engagement of the deep abdominal muscles is ignored, performance will be hindered. The crazy thing is I have watched efficiency (and movement quality) improve dramatically in yoga practitioners, golfers, and triathletes by simply improving the function of the deep stabilizing system. I have also seen grandparents pick up their grandchildren without pain, and low back pain lessen. Anatomy and physiology in the absence of disease is consistent- understanding how the body works dynamically is the most valuable tool a movement professional can have.
Your in health and wellness,
Jenn
P.S.- If you find this topic interesting and would like to study it further, I highly recommend Diane Lee's work (her website can be found at http://dianelee.ca/index.php) and/or the Postural Restoration Pelvis course (either home study or live).
Bordoni, B., & Zanier, E., (2013). Anatomic connections of the diaphragm: influence of respiration on the body system. Journal of Multidisciplinary Healthcare, 6, pp. 281-291.
Lee, D., (2011). The Pelvic Girdle, Fourth Edition. Churchill Livingston Elsevier: Toronto.