The little muscle that could, or why the serratus anterior is important for stabilization
I have come to the realization that I don't like the way anatomy is traditionally taught. During my undergrad, we went to the medical school at UC Davis, looked at prosections, and learned the muscles of each section- their actions, their origins, and their insertions. We never looked at how the body as a whole functioned to move, or approached anatomy the way I like to think of it now- these chains of muscles provide postural stability, these chains of muscles provide the strength necessary for movement, and here is how they interact (more anatomy trains-esque, although I am finding that understanding how to walk well is key to athletic performance. If you aren't walking efficiently, you aren't going to move efficiently during basketball, yoga, Crossfit, or whatever athletic endeavor you pursue). Prior to starting my graduate studies, I spent a weekend studying yoga with Kino MacGregor. She talked about "filling in the space between the shoulder blades" and activating the "serratus anterior." I was intrigued, both because it changed the way my plank felt and because it was a muscle I had heard of, but never given much thought to.
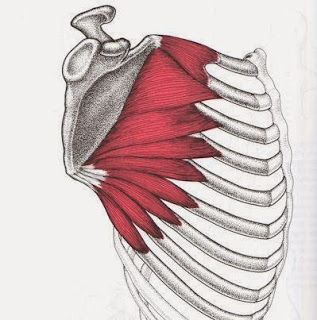
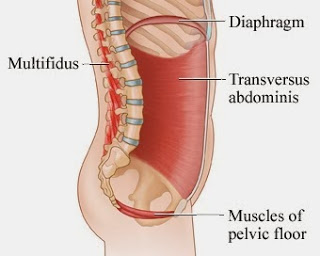
Fast forward four years: I have learned the serratus anterior is both critical for walking well, important for shoulder girdle stability, and begins the chain of muscles that stabilizes the core. The serratus anterior has attachment points on the front side wall of ribs 1-8 and the front surface of the scapula (http://www.anatomyexpert.com/structure_detail/5505/151/). It shares attachment points with the diaphragm, which has attachments at the xiphoid process, ribs, and lumbar spine. The diaphragm crura blends with the crura from the transverse abdominis; the diaphragm fascia also intertwines with the fascia from the psoas (Hatley, 2006). The serratus anterior (SA) protracts the shoulder blades and stabilizes the shoulder girdle and, like the transverse abdominimis, fires before you move to provide stability. The diaphragm is a muscle of inspiration and aids in postural stabilization. Its ability to properly dome up is based on the position of the rib cage (Hruska, 2005). This ultimately affects the ability of other muscles of the core to properly function, specifically the internal obliques and transverse abdominus. The transversus abdominus (TrA) is essentially the SA of the lumbar spine. It creates intraabdominal pressure and provides stability before movement, acting on a feed forward loop. The psoas flexes the hip and provides lumbar stability. Anteriorly and from a stability perspective, this links the shoulder to the hip in four steps. The interesting thing about all of these muscles is their ability to properly stabilize is position dependent. If you have scapula that are retracted in a resting position, your SA isn't in a good position. This is going to limit the ability of both the diaphragm and the TrA to properly function. If the scapulae are retracted, chances are high that during rest, the rib cage is in an inspiratory position, which will affect pelvis position. The ability of the deep stabilizers to work together is necessary for efficient movement mechanics, so while this started as a discussion of the oft forgotten serratus anterior, it's really a discussion of one piece of the deep stabilizing system.

Diaphragm Image
So how do we make sure it is working and why do we care? We care because if it's not stabilizing the shoulder girdle, something else has to, and usually that something else is the latissimus dorsi, rhomboids, and upper fibers of the trapezius. These muscles affect resting position of the scapulae, which is problematic if you raise your arms overhead for any reason. They also affect resting position of the pelvis, with an overactive latissimus tilting the pelvis anteriorly. This can also lead to a "pain in the neck," quite literally. Breathing should not take place with the shoulders elevating each inhale; when this happens, the upper trapezius and scalenes are going to be working overtime, which can cause overuse. This also means the diaphragm isn't working properly, which means the lumbar spine isn't being properly stabilized, which means the pelvic girdle isn't in an optimal position. In order to improve efficiency, the SA needs to be addressed.
The next question is how? First, we have to inhibit the overactive muscles and improve position, so the SA in a better position to do its job. If the scapulae are pulling away from the back, the scapulae retractors are working in over time. To stretch them, we are going to protract the scapulae and bring the rib cage back to meet the shoulder blades. Protraction also fires the SA, so we are killing two birds with one stone. Once the thoracic spine is less locked up and the scapulae are resting on the back, we can work on position. The medial borders of the scapula should be parallel to the spine at the level of T2-T7 and flush against the thorax (Osar, 2012). I use a tactile cue, which is demonstrated in the video below, but the key is to get the sense that the upper back is broad and the scapulae are gently being pulled down and around the back. This will inhibit the upper trapezius and activate both SA and the lower fibers of the trapezius, which relaxes the overactive muscles in the neck in people that are neck breathers. This needs to be done in order; skipping directly to lower trapezius/SA stability won't fix faulty shoulder position. The goal of all movement direction and cueing should be efficiency- how can we get the body to move well with the least amount of effort? This doesn't mean there won't be work; it simply means the body will work more cohesively, and ultimately perform better.
A quick side note- I find it is helpful to remember the shoulder girdle functions like the hip girdle. If we can relate the function of the muscles in the shoulder girdle to those in the hips, it sometimes makes things a little less foreign. I will be discussing this in an upcoming post.
Yours in health and wellness,
Jenn
Video link: http://youtu.be/KEqv3V9-htc
Hatley, S., (2006). Anatomy and Asana: Preventing Yoga Injuries. Eastland Press: Seattle
Hruska, R., (2005). ZOA position & mechanical function. Postural Restoration Institute, viii-xi (http://www.posturalrestoration.com/resources/dyn/files/1051512z69443dbe/_fn/ZOA.pdf)
Osar, E., (2012). Corrective Exercise Solutions to Common Hip and Shoulder Dysfunction. On Target Publications: Aptos.